Multiple myeloma is a neoplastic disease characterized by infiltration of bone and bone marrow by myeloma cells forming multiple tumor masses that lead to pathological fractures. The condition is usually progressive and fatal. Symptoms include anemia, renal damage, and high globular levels in blood and increased susceptibility to bacterial infections. The impaired abnormal immunoglobulin production observed in multiple myeloma may be due to the presence of a monocyte or macrophage that suppresses the maturation of normal B-lymphocytes into Antibody secreting plasma cells. Life expectancies are related to the extent of the disease at diagnosis and response to treatment. Median life expectancy of responding patients is two to three years. High levels of M protein in serum or urine, bone lesions, hypercalcemia, pancytopenia, and renal failure are unfavorable signs.
Review
The patient is a 56-year-old white male, a retired supervisor at a nuclear energy plant, in previous good health. He initially presented to the office on September 30, 1998, complaining of tiredness, weakness, general malaise, abdominal discomfort, productive cough, and was concerned about attending his daughter’s wedding.
Physical examination revealed a 56-year-old white male with chronic low back pain, sinusitis, bronchitis, mild anemia, and in no acute distress. A non fasting comprehensive metabolic profile (chem12), amylase, lipase, lipid profile, thyroid screen and complete blood count (CBC) were ordered and the patient was instructed to visit the hospital laboratory. Initial evaluation of the chemistry results showed an elevated total protein of 13.1 g/dl with normal albumin level of 3.5 g/dl. The BUN and creatinine results were elevated at 54 mg/dl and 3.2 mg/dl respectively. Other abnormal chemistry results were potassium 5.3 mmol/L, chloride 109 mmol/L, calcium 12.8 mg/dl and phosphorus 5.4 mg/dl. The protein result was repeated and the original result was confirmed. Initial CBC was unremarkable aside from mild anemia (hemoglobin 10.3 g/dl and hematocrit 31.2%) with a normal WBC of 7.17×103/cmm and platelet count of 269×103/cmm. Reflex testing of immunoglobulins was performed and the laboratory report indicated that the IgA value was elevated at 6020 mg/dl with a depression of the IgG of 266 mg/dl and IgM of 37 mg/dl. Protein electrophoresis was ordered and a sample was sent to the reference laboratory for analysis. The protein electrophoresis confirmed the presence of a M-spike in the gamma region. Immunofixation revealed an IgA kappa monoclonal immunoglobulin detected along with free monoclonal kappa light chains. Suppression of IgG and IgM was confirmed by the reference laboratory. Radiologist review of the abdominal series performed during the initial evaluation revealed degenerative changes of the lumbar spine with disc degeneration at the mid and lower lumbar levels, no acute abdominal abnormality, and symmetrical hyperinflation consistent with obstructive airway disease. No acute cardiopulmonary disease was evident.
The patient was referred to an oncologist in Augusta Georgia and during a subsequent visit to the county hospital on December 23, 1998 for laboratory testing it was determined that his hemoglobin and hematocrit had fallen to 8.4 g/dl and 26.7% respectively with a normal WBC of 7.13×103/cmm and platelet count of 274×103/cmm. His oncologist initiated a standing order for a two-unit crossmatch whenever the hemoglobin dropped below 9.0 g/dl and two units were administered during this visit. He continued to visit his oncologist in Augusta Georgia and was also referred to a clinic in Arkansas for further evaluation and treatment.
In February 1999 his hemoglobin dropped below 8.8 g/dl and he was given two units of packed red blood cells. At this time his platelet count was still normal at 478×103/cmm. During the second half of February he underwent the first of three unsuccessful bone marrow transplants. The initial post transplant WBC was 0.5×103/cmm with a hemoglobin of 8.9 g/dl, hematocrit of 27.3% and platelet count of 65×103/cmm. Despite repeated transfusions of packed red blood cells and platelet pheresis packs as well as Procrit and Neupogen treatments his red blood cell and platelet counts continued to decline. Renal function continued to deteriorate over the next several months as measured by BUN and creatinine which were higher at 70 mg/dl and 4.8 mg/dl respectively. He developed mild acidosis and his potassium continued to rise to a high of 6.9 mmol/L. Total protein was normal at 6.8 g/dl. The CBC demonstrated a WBC of 2.95×103/cmm, hemoglobin 10.0 g/dl, hematocrit 29.3% and platelet count of 44×103/cmm.
On September 8, 1999, the patient visited this office with a productive cough with rhonchi. A pa and lateral chest film was ordered and the results were compared to films made one year earlier on September 30, 1998. The chest films were reviewed by the radiologist. His report indicated, right medial basilar bronchietatic change with atelectasis and bronchial wall thickening which has developed since the last examination. Bronchial wall thickening may reflect active bronchial inflammation. No focal air space infiltrate was demonstrated. Laboratory evaluation revealed continued mild anemia, hemoglobin 9.3 g/dl and hematocrit 27.5% with a WBC of 4.21×103/cmm and continued decreased platelet count of 42×103/cmm. There were no additional visits until after the patient returned from an extended trip to Arkansas for the final bone marrow transplant.
The patient visited the hospital laboratory for evaluation, on November 5, 1999, after the last bone marrow transplant. Protein electrophoresis performed during this visit revealed a decrease Total protein and albumin, 5.5 g/dl and 3.0 g/dl respectively and the electrophoretic interpretation was essentially normal. Urine protein electrophoresis revealed no abnormal urine protein. Creatinine clearance was 24.8 ml/min with a micro protein of 33 mg/dl. BUN and creatinine values had remained elevated and were now 99 mg/dl and 4.7 mg/dl respectively. Hematology results were as follows; hemoglobin 8.8 g/dl, hematocrit 25.8%, WBC 4.54×103/cmm and platelet count 23×103/cmm. Throughout the remainder of November and December in spite of multiple PRBC and platelet transfusions the platelet count remained at or below 25×103/cmm with hemoglobin at or below 9.5 mg/dl.
The patient continued to lose weight and reached a low of 140 lbs. from an original weight at diagnosis of 175 lbs. In late December, he presented at the emergency department and was transferred to Doctor’s Hospital in Augusta, Georgia with a low grade fever, pneumonia and possible sepsis. Additional symptoms were shortness of breath, cough, diarrhea, nausea, vomiting and anorexia. Sputum and blood cultures performed on admission to the referral facility were positive for Vancomycin resistant Staphylococcus aureus. He remained in the hospital for seven days, after which, he was instructed to return home to “get his affairs in order,” with a diagnosis of multiple myeloma unresponsive to three bone marrow transfusions and Vancomycin resistant Staphylococcus aureus pneumonia.
Of major significance at the time was the patient’s morale. He requested that the family leave him alone to die and was now bedridden and housebound. On presentation of the patient’s wife and daughter and because of previous discussions of the application of alternative medicine in this case and the desire of the patient and family to try anything a program of alternative therapy was prescribed. The patient began a daily regimen of what we have termed an “alternative MOP therapy”:
Beta-1,3-D glucan 500mg T.I.D.
MAK-4 1 tsp. T.I.D.
MAK-5 1 tablet T.I.D.
Pro-Boost Thymic formula 1 packet sublingual T.I.D.
Gerovital GH3 1 tablet T.I.D.
Maitake mushroom extract 2 droppers full T.I.D.
In order to insure that he met minimum nutrient targets his diet included daily portions of fresh fruits, vegetables, and supplementation with a liquid protein supplement as tolerated. Along with these oral medications counseling to reinforce the need for a positive mental attitude and guided imagery to see himself well was also included in the protocol. To his credit he was extremely compliant and followed the alternative clinical protocol as directed religiously.
Within a period of one week ulceration of the mouth had resolved and the patient was somewhat better in appearance and was ambulatory. Laboratory results indicated that the BUN and creatinine were slightly lower and his electrolyte status was improved although he continued to be acidotic. All laboratory results during this period were copied and sent to his physicians in Augusta and Arkansas. He also maintained a positive mental attitude. During January and early February, 2000 the patient continued exclusive treatment with the alternative therapies and traveled to the clinic in Arkansas for follow-up. It was during this visit that it was determined that the patient was “miraculously in remission and without pneumonia.” Upon his return home the patient insisted on continuation of the alternative therapy. The platelet count began to rise in the second half of February and during the last week of February the oncologist began therapy with Thalidomide. Subsequent platelet counts began to drop and the Thalidomide therapy was discontinued. Platelet counts again began to rise and during the last week of March 2000 the platelet count rose above 50×103/cmm for the first time in more than six months. BUN and creatinine results had dropped to 50 mg/dl and 3.2 mg/dl respectively and protein/albumin results were now normal.
He began to improve significantly and resumed many of his former activities. During this period of well being he decided without notifying either his physicians or family, to decrease his medications and within a period of two weeks his laboratory results began to reflect a slide in his condition. He was counseled as to the necessity to maintain the clinical protocol as instructed and again after a short period of optimum compliance his health and laboratory results began to improve.
The electrolyte status is currently normal as well as CBC and differential and globulin levels. He has resumed many of the activities he was accustomed to prior to diagnosis to include favorite pastimes of driving, fishing, playing golf, visiting friends, and eating out.
Discussion
A greater number of Americans are turning to alternative therapies for the treatment of a wide variety of health conditions either as a way to enhance their traditional medical care as a substitute for conventional methods of treatment. Patients seek alternative therapies to promote wellness, to enhance the quality of their lives, or to practice disease prevention. In order for an alternative therapy to truly qualify as integrative or complementary we feel it must meet three basic criteria:
It should not interfere with any traditional therapy the patient may already be receiving
It should provide protection from the toxic effects of the traditional therapy the patient is receiving
It should be capable of supporting the patient as a stand alone therapy.
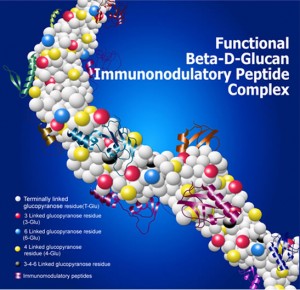
In this patient’s treatment we thought that since the macrophage plays an essential role in initiation and maintenance of the immune response we would target our alternative therapy at stimulating macrophage activity. The macrophage is the oldest and most consistently preserved immunologically a competent cell known. The macrophage must be activated, a process involving a number of morphological changes, in order to function defensively. In addition, a cascade of metabolic changes occur resulting in the production of a number of cytokines which in turn act as internal regulators of the immune system. Macrophage stimulation or activation can be initiated by a variety of different stimuli such as endotoxin, bacteria, viruses or chemicals. However, these activators can be too toxic or pathogenic to be medicinally useful. Beta-1,3-D glucan on the other hand is orally effective, completely safe and non-toxic and is a very powerful stimulator of the immune response.(1) Not all types of beta glucan are physiologically active. Beta-1,3-D glucan derived from the cell wall of yeast is probably the most physiologically active form, and in addition to beta-1,3-D glucan, a broad spectrum glucan source, the Maitake extract(2) was added. A three dimensional model of beta-1,3-D glucan shows it to be a helix, and research at Harvard University has shown that receptors for approximately seven sugar residues exist on the macrophage cell membrane.(3) The fact that such a small number of glucose units can activate these receptors and that there are specific receptors for this sort of polysaccharide chain on the surface of the most ancient cell in the immune system is very remarkable.(4) There is now evidence to show that beta glucan may be the most ubiquitous macrophage activator in nature. Once activated the macrophage, through its ability to initiate a cascade of cellular responses, becomes the central conductor of the immune symphony. A macrophage can recognize and kill tumor cells nonspecifically, as well as remove foreign debris. When activated by the combination of beta-1,3-D glucan and Maitake extract, the macrophage produces either directly or through stimulation of additional cells a number of essential cytokines (IL-1, IL-2, IL-6, TNF and INF) that are able to stimulate the immune system and boost bone marrow production.
Research has established that glucans provide a protective effect against an extensive list of microorganisms to include: Staphylococcus aureus, Eschericia coli, Candida albicans, Pneumocystis carinii, Listeria monocytogenes, Leishmania donovani, Herpes simplex, Ascaris sp. Numerous studies support the theory that an antibiotic and a macrophage activator, such as glucan, work synergistically. Experimental peritonitis in rats was used to show a synergy between the widely used antibiotic ampicillin and glucan. A 100% survival was the result of the combination treatment, while glucan alone gave 30% survival, and ampicillin in the given dose elicited 65% survival (20% survival in the control group). All the results were statistically significant.(5),(6)
The protective effect of yeast glucan on bone marrow in radiation therapy is well established and documented with the mechanism of enhancing hemopoietic recovery and by regenerating the host’s ability to resist life-threatening opportunistic infections.(7) However, it also has been demonstrated that host resistance to opportunistic infection in glucan-treated irradiated animals is enhanced even prior to the detection of significant hemopoietic regeneration. This early enhanced resistance to a microbial invasion could be correlated with enhanced and/or prolonged macrophage, but not granulocyte, function.
Experimental data suggest that glucan can also function as an effective free-radical scavenger (primarily toward hydroxyl radical). Because the macrophage has been shown to selectively phagocytize and sequester glucan, it is possible that these specific cells may be protected by virtue of glucan’s free-radical scavenging ability.(8) Oral application of yeast beta-1,3-D-glucan for 20 consecutive days after a single, near lethal, dose of radiation resulted in 70-90% survival versus 30% in the control group.
Another aspect of glucan therapy is it’s ability to also protect a patient from leukocytopenia associated with chemotherapy. Studies have shown that oral administration of glucan can prevent the decrease in the number of peripheral leukocytes induced by the administration of 5-fluorouracil. Proliferative responses of bone marrow cells to granulocyte/macrophage colony stimulating factor (GM-CSF) or granulocyte colony stimulating factor (G-CSF) were suppressed by the administration of 5- fluorouracil, and their recoveries were enhanced by glucan and serum levels of cytokines such as IL-1 and IL-6 were increased.(9)
In addition, thymic protein plays a pivotal role in the programming of immature T-4 cells and it is necessary to provide supplementation of this gland. Thymic Protein, an “intact” 500 amino acid chain which fits the receptor site on the T-4 cell, successfully programming the T-4 cells, sets off a cascade of cytokine and lymphokine formation and release.(15) The released cytokines and lymphokines act as messengers to further stimulate target cells to attack and destroy certain invading pathogens. The activated T-4 helper cells also stimulate bone marrow to produce white blood cells, red blood cells and specific CD56 natural killer cells which play a key role in the destruction of cancer cells.
In summary it has been two years since the initial diagnosis of Multiple Myeloma. The combination of immunostimulants, antioxidants, and thymic protein replacement therapy showed:
Remission of multiple myeloma
Resolution of Vancomycin resistant Staphylococcus aureus pneumonia
Absence of toxic side effects of alternative treatments
Improvement in longevity and in quality of life
Comparatively inexpensive treatment.
References:
1. The formulation of beta 1,3-D glucan used was the Beta Right™ brand manufactured by A. J. Lanigan, (877) 407-3999
2. Maitake mushroom D-fraction™ manufactured by Maitake Products, Inc. New Jersey, (201) 229-0101
3. Zymosan, the cell wall from Saccharomyces cerevisiae, was reported to be a macrophage activator through its beta-glucan over 30 yr ago. Nevertheless, the identity of the beta-glucan receptor has been controversial. This study showed that the alpha M beta 2-integrin, CR3 (Mac-1, CD11b/CD18) served as the beta-glucan receptor through one or more lectin sites located outside of the CD11b I-domain that contains the binding sites for iC3b, ICAM-1, and fibrinogen.
4. Thornton BP; Vetvicka V; Pitman M; Goldman RC; Ross GD; Department of Pathology, University of Louisville, KY 40292, USA.; J Immunol, 156: 3, 1996 Feb 1, 1235-46
5. Research Summary; “Beta 1,3-D Glucan Activity in Mice: Intraperitoneal and Oral Applications, ” Baylor College of Medicine 1989.
6. Glucan-based macrophage stimulators may prevent infections in trauma and surgical patients Reported from Drug & Therapy Perspectives 1996 Aug 19; 8(4): 6-7
7. Research report; “Radioprotective Effect of Oral Administration of Beta 1,3-D glucan.” Armed Forces Radiobiology Research Institute, Bethesda, MD, 1987.
8. Patchen M.L., Alesandro M.M., Brook I., Blakely W.F. McVittie T.J., Glucan: Mechanisms Involved in Its Radioprotective Effect J Leuc Biol.; 42:95-105.
9. Miyazaki 1992
10. Gerovital GH3, distributed by Nutriceutics Corporation, Florida, (800) 391-0114.
11. Amrit™, Maharishi Amrit Kalash, by Maharishi Ayurvedic Products International, Inc., Colorado, (800) 255-8332.
12. The Amrit Protection MAK-4 formula significantly induced morphological differentiation (neurite formation) and biochemical differentiation (a 15-fold increase in tyrosine hydroxylase activity) in 75% of neuroblastoma cells in culture. This is indicative of a reversal of the malignant process.
13. Journal of Applied Nutrition, Vol. 48, Nos. 1 and 2, pp. 10-21, 1996
Love and Light
The Healing Oracle Team
Please join our growing numbers on MeWe: Healing Oracle
Also join us on Twitter | YouTube
Global Petition
Please sign our global petition against enforced vaccinations The intention of this petition is to present 5 million signatures to each President, Prime Minister, Health Minister and heads of state worldwide.
Vaccines are a global problem and need to be tackled on a global level.
If we stand as one, we have a chance of saving the children of the future.